On Monday 14th March I volunteered to take part in a focus group considering how best to involve patients in the development of new drugs. Patient involvement in research seems to be a growing interest nationally and also chimes well with the mission statement of Derriford Hospital – putting the patient first.
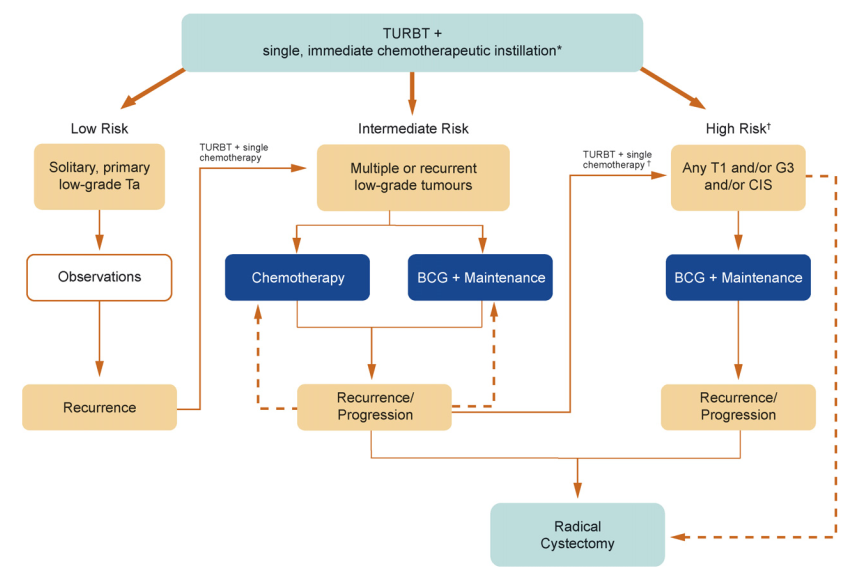
The study is being undertaken at the University of Kent and links specifically to the development of a new drug to be used in conjunction with Mitomycin after TURB-T to increase its effectiveness in the treatment of non-invasive, high risk bladder cancer. Patient involvement would not be as guinea pigs but rather as end users who might have useful contributions on the administration of the drug, any side effects and outcomes.
In a Teams meeting with other patients being treated for bladder cancer and two researchers from the University of Kent we discussed a series of questions including whether we, as individuals, would be interested in taking part in the research, how much we understood about drug research and clinical trials, why patient involvement might be useful, how we might wish to be involved (face-to-face meetings, on-line, in print, etc) and what we expected to get out of it.
The discussion highlighted our different experiences of support and engagement with support organisations. At different stages of treatment from different backgrounds and from different parts of the country we all declared an interest in being involved and expected no remuneration because we all felt that we personally might benefit and others certainly would and that would be reward enough. Hopefully I will continue to be involved in this research and be able to share elements of it with our group.
If you are in the United Kingdom and have non-muscle invasive bladder cancer (NMIBC), previously known as superficial bladder cancer, you may be eligible to take part in our paid telephone/online interview. If you have a friend/relative who has NMIBC, please share this advertisement with them, as they could be eligible to take part in our paid telephone/online interview.
We are trying to find out about the aspects of treatment that matter to patients with NMIBC. Can you help? You can make your voice heard about your treatment priorities by taking part. Eligible participants will be paid £80 for completing the interview and £30 for providing proof of their diagnosis. The interview, including a brief online survey, will last up to 60 minutes.
If you are interested in participating or would like to receive further information about the study, please feel free to contact Nadine on nadine.koekemoer@evolve-fieldwork.com.
If you are in the United Kingdom and have non-muscle invasive bladder cancer (NMIBC), previously known as superficial bladder cancer, you may be eligible to take part in our paid telephone/online interview. If you have a friend/relative who has NMIBC, please share this advertisement with them, as they could be eligible to take part in our paid telephone/online interview.
We are trying to find out about the aspects of treatment that matter to patients with NMIBC. Can you help? You can make your voice heard about your treatment priorities by taking part. Eligible participants will be paid £80 for completing the interview and £30 for providing proof of their diagnosis. The interview, including a brief online survey, will last up to 60 minutes.
If you are interested in participating or would like to receive further information about the study, please feel free to contact Nadine on nadine.koekemoer@evolve-fieldwork.com.
Alternatively you can leave your contact detail via the following link and we shall get in to contact with you: https://forms.gle/ZZvp1MM6p83fCy6R7
A new technique for analysing tumours called “representative sequencing” is reported in several papers this week. It could be available in the NHS within 3 years. It offers a means of more thorough analysis of a tumour and therefore more accurately identify the appropriate treatment. The results were published in the journal Cell Reports but a brief summary taken from the “i” newspaper is here https://inews.co.uk/news/health/tumour-analysis-personalised-cancer-care-nhs-explained-2843531
May is the month for raising awareness of bladder cancer. On their website the World Bladder Cancer Patient Coalition has produced a toolkit of information on the world wide picture. You may want to take a look at its colourful pages
There is no evidence that the Bacille Calmette-Guérin vaccine (BCG) protects people against infection with COVID-19 virus. Two clinical trials addressing this question are underway, and WHO will evaluate the evidence when it is available. In the absence of evidence, WHO does not recommend BCG vaccination for the prevention of COVID-19. WHO continues to recommend neonatal BCG vaccination in countries or settings with a high incidence of tuberculosis.1
There is experimental evidence from both animal and human studies that the BCG vaccine has non-specific effects on the immune system. These effects have not been well characterized and their clinical relevance is unknown.2,3
On 11 April 2020, WHO updated its ongoing evidence review of the major scientific databases and clinical trial repositories, using English, French and Chinese search terms for COVID-19, coronavirus, SARS-CoV-2 and BCG.
The review yielded three preprints (manuscripts posted online before peer-review), in which the authors compared the incidence of COVID-19 cases in countries where the BCG vaccine is used with countries where it is not used and observed that countries that routinely used the vaccine in neonates had less reported cases of COVID-19 to date. Such ecological studies are prone to significant bias from many confounders, including differences in national demographics and disease burden, testing rates for COVID-19 virus infections, and the stage of the pandemic in each country.
The review also yielded two registered protocols for clinical trials, both of which aim to study the effects of BCG vaccination given to health care workers directly involved in the care of patients with COVID-19.4,5
BCG vaccination prevents severe forms of tuberculosis in children and diversion of local supplies may result in neonates not being vaccinated, resulting in an increase of disease and deaths from tuberculosis.6-8 In the absence of evidence, WHO does not recommend BCG vaccination for the prevention of COVID-19. WHO continues to recommend neonatal BCG vaccination in countries or settings with a high incidence of tuberculosis.
We asked our CNS what the impact of Covid-19 has been on the Unit. These answers we hope you will find helpful. Where possible clinics are carried out by phone. If you are invited into the Unit you will be telephoned 24 hours before the appointment to confirm that you are well enough to visit and are still willing to come into Derriford. Whether you are a new patient or an existing one you still arrive and leave the Unit by the single entrance but when you come in your temperature will be checked. Staff temperatures are checked daily. Staff and patients wear PPE where face to face contact is necessary.
Telephone clinics reduce footfall into the hospital, therefore reducing clinical risk for patients and staff.
For new patients Assessments for bladder, kidney and prostate symptoms are still being carried out but results are given by phone and letter. For bladder cancer patients TUR-BTs are still being carried out but at Care-UK rather than Derriford. Pre op assessment along with COVID 19 swabs are done at Care UK. Bigger operations such as nephrectomies and cystectomies are still going ahead at Derriford. Pre op assessments/COVID 19 for these patients take place at Derriford. Lynher ward has moved. Post op patients are nursed on Stonehouse Ward at present.
For existing patients Cystoscopies are still being carried out on time and in the Unit. BCG and mitocycin treatments are being administered only to high risk patients. Other treatments are deferred. Chemotherapy is being offered on a reduced service by Oncology which is operating out of the Nuffield Hospital across the road.
What contribution can patients make to saving lives? Follow the goverment advice and any directions of the hospital on your visit. Stay safe.
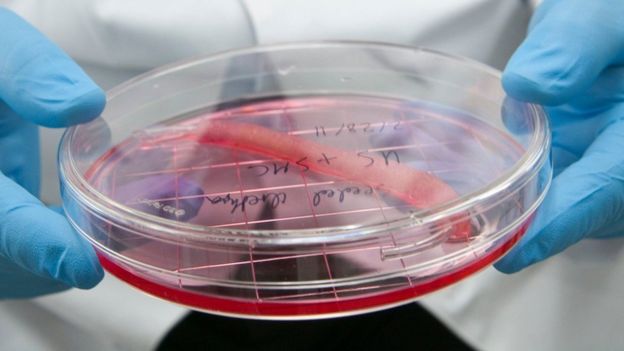
Bioprinting human tissue using specialised 3D printers promises to transform medicine, with implications for organ transplants, cancer treatment and antibiotic development.
Luke Massella is one of about 10 people alive walking around with a replacement bladder that has been grown from his own cells.
He was born with a condition called spina bifida, which, from birth, left a gap in his spine.
By 10 years old, he had survived a dozen surgeries and beaten doctors’ initial expectations that he’d never walk. But then a malfunctioning bladder made his kidneys fail.
“I was kind of facing the possibility I might have to do dialysis [blood purification via machine] for the rest of my life,” he says. “I wouldn’t be able to play sports, and have the normal kid life with my brother.”
An enterprising surgeon, Anthony Atala at Boston Children’s Hospital, took a small piece of Luke’s bladder, and over two months grew a new one in the lab.
Then in a 14-hour surgical procedure he replaced the defective bladder with the new one.
“So it was pretty much like getting a bladder transplant, but from my own cells, so you don’t have to deal with rejection,” says Luke.
Rejection is when the body’s immune system attacks transplanted cells that come from another organism. Using tissue grown from a patient’s own cells helps combat this effect.
Luke went on to be a wrestling coach in the Connecticut public schools and now, at 27, runs events in the jewellery industry.
“Pretty much I was able to live a normal life after,” he says.
He underwent surgery 17 times before he was 13, but hasn’t had to since.
Dr Atala’s work involves bioprinting, using modified 3D inkjet machines to produce biological tissue.
His team has developed “eight cell-based tissues we put into patients,” he says, including engineered skin, urethras, and cartilage, all grown in the lab.
These engineered organs are going through clinical trials for approval by the US Food and Drug Administration.
“You need to know how to make these organs by hand, then the bioprinter is really a scale-up tool,” says Dr Atala, director of the Wake Forest Institute for Regenerative Medicine in North Carolina.
In other words, bioprinting would enable these organs to be made in an affordable, consistent, and precisely constructed way, he believes.
“Flat structures like skin” are easiest to print, he says. Then “tubular structures like blood vessels and urethras” are a little more complex, with “hollow non-tubular organs like bladders” harder still.
But hardest are “solid organs like hearts, lungs, and kidneys,” with “so many more cells per centimetre”.
For these highly complex organs bioprinters provide a precision that surpasses human hands, he says.
Pluripotent potential
Bioprinting has taken off following a dramatic discovery by Shinya Yamanaka and Sir John Gurdon, who a Nobel Prize for their work in 2012.
Adult ordinary cells can now be reprogrammed to make stem cells – called induced pluripotent stem cells – which can be used to make any other cell in the body.
“A lot has happened in the last couple of years,” says Steven Morris, chief executive of bioprinting start-up Biolife4d.
Mr Morris is working to bioprint a heart using these pluripotent cells over the next year. This will initially be a smaller version of the organ, he explains, but could eventually help pharmaceutical companies bypass testing trial drugs on animals, he says.
And ultimately, bioprinting organs from people’s own cells will solve the “huge lack of supply” in organs for transplant, says Mr Morris, and do away with the need for anti-rejection immunosuppressant drugs.
Specialist printers could even reproduce cancers tumours, giving doctors the chance to test “which treatment could specifically work on that patient,” says Erik Gatenholm, chief executive of Swedish start-up Cellink.
His firm has been given a €2.5m ($2.9m; £2.2m) grant from the European Union to develop these tumour-modelling printers.
Bioprinters also give us a way of “quickly laying down small quantities of fluid to test if a new antibiotic would work for that specific patient,” says Annette Friskopp, vice president for specialty printing systems at the large tech firm HP in Palo Alto.
This could help tackle the growing and serious problem of antimicrobial resistance – the rise of “superbugs” traditional antibiotics can’t kill.
HP is partnering with the US Center for Disease Control to deploy printers in four regional labs in the US this autumn.
Inks and scaffolds
Printers of any kind need ink, and bioprinters are no different. “Bioink” is a gel that can be extruded through a printing nozzle and mimics the suspension lying between cells, called the extracellular matrix.
Both university labs and start-ups, such as Cellink, have been developing bioinks that can be used with many types of cells, says Ahu Arslan Yildiz, a biochemist who heads a research group at Izmir Institute of Technology in western Turkey.
And these “universal” bioinks are growing more and more “processable and easy to handle,” says Ms Yildiz, while also not being toxic.
Another breakthrough in the fast-developing field comes from Japan.
Most bioprinting uses a scaffold to hold cells in place. And once cells are “coaxed to a certain level, they begin to self organise and assemble,” says Arnold Kriegstein, director of the stem cells and regeneration medicine centre at the University of California, San Francisco.
They hope it will lead to more patients being cured while experiencing fewer side-effects.
Barry Dolling, 65, who has prostate cancer, is the first patient in the UK to be treated.
He told me: “I feel privileged and excited to be part of this. I volunteered to be part of the Prism trial and feel my treatment and the research will help others diagnosed with prostate cancer in the future.”
Pioneering
Prof Uwe Oelfke, who leads the joint MR Linac project at the ICR and Marsden, told me: “Ten years ago we did not think it would be possible to combine MRI and radiotherapy – this is a real step-change in technology.”
The machine has been specially designed so that the magnetic coils of the MRI and the X-ray beam of the linear accelerator do not interfere with each other.
It will be especially useful in treating tumours that shift in size and shape in the body, such as in the lung, bladder and bowel.
Dr Alison Tree, consultant oncologist at the Royal Marsden, described the new technology as “a dream come true” that would enable clinicians to deliver more targeted, higher doses of radiation, sparing healthy tissue.
“In lung cancer, we would like to give higher doses of radiotherapy but are limited because the tumour is often close to other vital structures in the chest,” she said.
“This allows us to see the cancer more clearly and make sure the radiation goes where it is needed and not where it can cause harm.”
Single treatment
The ability to give higher doses of radiation will enable patients to complete their treatment more quickly.
Mr Dolling will have 20 sessions of radiotherapy in the MR Linac. But it’s predicted that eventually it will be possible to cure some cancers in a single treatment.
The Royal Marsden will treat prostate, rectal, bowel, bladder, cervical and eventually lung cancer in the MR Linac.
The installation of the MR Linac was made possible by a £10m grant from the Medical Research Council, plus support from the Royal Marsden Cancer Charity.
A second machine, at the Christie in Manchester, will begin treating patients early next year.
Both hospitals are part of an international research consortium together with companies Elekta, which makes the MR Linac, and Phillips.
So far, the only other cancer centres to treat patients with the MR Linac are in the Netherlands, in Utrecht and Amsterdam.
The prospect of more accurately targeted radiotherapy, with fewer side-effects, will inevitably mean there will be high demand for access to treatment in the MR Linac.
Dr Tree said there would be several clinical trials and priority would be given to research that yielded the most benefit to patients.
There have been significant improvements in radiotherapy treatment in recent years – it already contributes to 40% of all the cases of cancer that are cured.